 |
| Ageing hands at the piano |
Context of piano playing injuries:
The more you play (and the higher level you play at) the more likely you are to become injured. LINK (2010) - p.61. Prevalence of ongoing injuries in professional musicians seems to be greater than 50%.
Piano players' common occupational ailments LINK (2010) - p.62
1) Tendinitis - inflammation of tendons
2) Overuse syndrome / RSI (not necessarily an accepted diagnosis) - degeneration of tendons/ligaments/nerves as rate of injury > rate of healing; LINK
3) Carpal tunnel syndrome - median nerve trapping in the carpal tunnel of the wrist
4) Radial nerve compression syndrome - particularly entrapment of radial nerve at elbow
5) + Osteoarthritis - degenerative changes to hand/wrist joints due to overuse LINK (1984)
Abducted (splayed out) fourth and fifth fingers most likely to be damaged LINK (1989) - p.108
Extended wrist play causes damage, as do fortissimo and octave play LINK (1998) - p.11
Treatments
NB: these are remarkably similar to one another
1) Tendinitis: avoid rapid increase in tendon use; splinting and rest; painkillers; steroid injections.
2) Overuse syndrome: rest and anti-inflammatories; + potential use of ?quack massage therapy (ART) which describes a rather simplistic pathophysiology LINK
3) Carpal tunnel syndrome: splinting and rest; steroids; carpal tunnel release surgery LINK
4) Radial nerve compression: splinting and rest; steroids; surgical release of nerve along its course LINK
5) Osteoarthritis: rest, pain-based treatment and potentially joint replacement LINK
Additional advice
> Most piano-playing hand disorders are due to the mechanical process of learning and playing; non-expert doctors are ill-equipped to be able to offer helpful advice about how to resolve these problems; experienced piano teachers are more likely to be able to do so based on their own experience LINK
> Resting within and between practice sessions enables removal of metabolic waste products and replenishment of phosphocreatine, ATP, acid/base balance, resting membrane potentials ?weak LINK> Resting during practising also enhances procedural memory retention LINK
> If you're overstretching with your small hands, you can either pick tunes with smaller spans, or there are people out there who'd like to sell you a smaller-size ergonomic piano, sounds sensible enough, if a little inconvenient to transport to performances! LINK
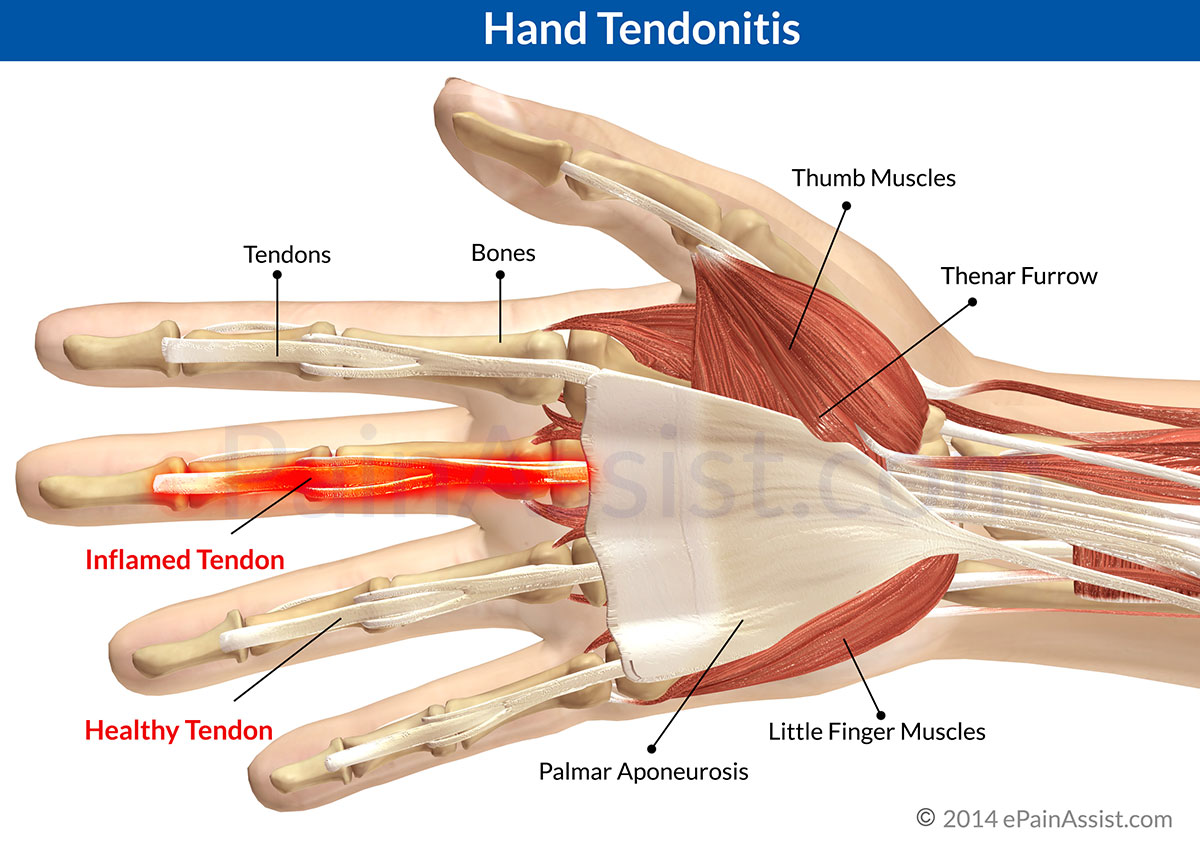 |
| Tendinitis in the hand LINK |
 |
| Carpal Tunnel Release |
 |
| Joint changes in osteoarthritis of the hands LINK |
 |
| 'Play Me I'm Yours' street piano duet - Toronto |



